This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
A 45 years old male,daily wage worker, father of 4 children came with the cheif complaints of generalised weakness since 2 months
Irregular to work(due to generalised weaknesses since 16 years) but used to walk without support (used to ride bicycle stopped as he developed giddiness) and developed sensation of both lower limbs.
H/o fall from tree, due to slippage at age of 12 years -- developed hearing loss and tinnitus since then
Developed swelling of scrotum and low backache 4 years ago and underwent surgery for hydrocele, and diagnosed to be having diabetes since 4 years (not used any medication)
6 months ago developed scaly hyperpigmented papules -itchy lesions initially developed in bilateral lower limbs and then spread upwards and involved bilateral lower buttocks and lower abdomen (acquired from his wife)
C/o hard stools associated with bleeding per rectum since 2 months
2 months back h/o outside food intake , developed vomiting (for 1 day) and developed gradually progressive, weakness of both lower limbs (associated with decreased sensation of lower limbs and upper limbs)
K/c/o diabetes since 4 years (not on any medication
N/k/c/o diabetes, hypertension, TB, ba, epilepsy, thyroid
H/o hydrocele surgery 4 years ago
Personal history: labourer by occupation
Habits: smoker: 30 years ago
General physical examination:
Patient is c/c/c
No signs of pallor icterus cyanosis clubbing genralised lymphadenopathy and pedal edema
Temp: afebrile
Pr: 86bpm
RR: 14 cpm
BP: 110/70mmhg
GRBS:172mg/dl
Systemic examination:
Cvs: s1 and s2 heard. No murmurs
Rs: b/l ae present. Nvbs
P/a: soft. Non tender
CNS:
UPPER LIMB LOWER LIMB
TONE
RIGHT HYPO. N
LEFT. HYPO. HYPO
POWER
RIGHT. +4/5. 5/5
LEFT. -4/5. -4/5
REFLEXES:. RIGHT. LEFT
BICEPS. -- --
TRICEPS -- --
SUPINATOR. -- --
KNEE. -- --
ANKLE. -- --
PLANTAR. Mute. Mute







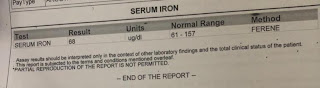
INVESTIGATIONS:














Rx:
1. INJ. OPTINEURON IN 500 ML ND IV/OD
2. TAB. GABA NT 100/10 MG PO/H/S
3. TAB. RANTAC 150 MG PO/OD
4. PHYSIOTHERAPY OF UPPER LIMB AND LOWER LIMB

Comments
Post a Comment